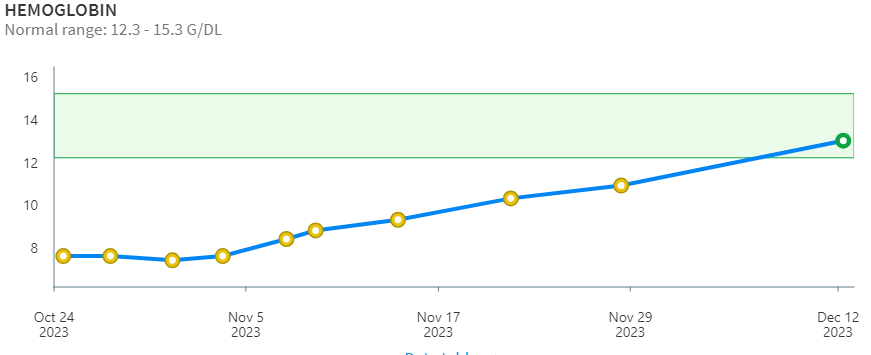
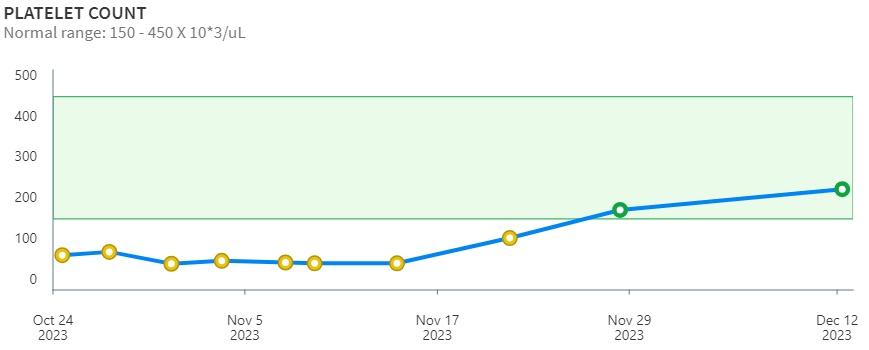
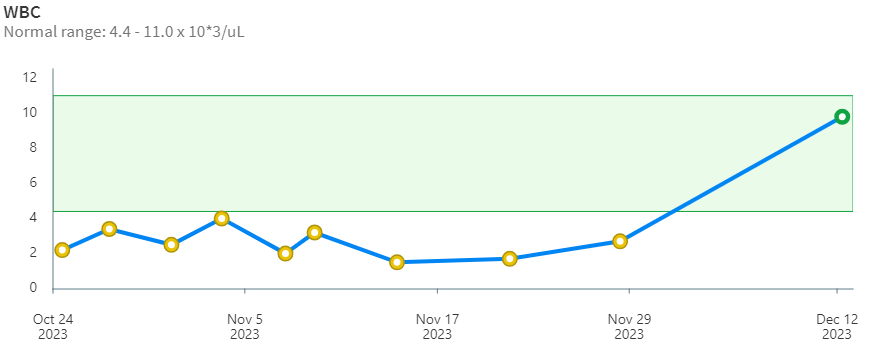
I am on elotuzumab, dexamethasone, and pomalidomide now. I am in my second cycle. It’s been working great. My CBC is better than it’s been in years. Here are my most recent results in graph form.
Beth Morgan Multiple Myeloma Treatment Blog
My life as a myeloma patient for almost two decades
This is from medline plus:
http://www.nlm.nih.gov/medlineplus/druginfo/uspdi/202018.html#SXX20
Along with its needed effects, a medicine may cause some unwanted effects. Although not all of these side effects may occur, if they do occur they may need medical attention. When this medicine is used for short periods of time, side effects usually are rare. However, check with your doctor as soon as possible if any of the following side effects occur:
Additional side effects may occur if you take this medicine for a long time. Check with your doctor if any of the following side effects occur:
Other side effects may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. However, check with your doctor if any of the following side effects continue or are bothersome:
After you stop using this medicine, your body may need time to adjust. The length of time this takes depends on the amount of medicine you were using and how long you used it. If you have taken large doses of this medicine for a long time, your body may need one year to adjust. During this time, check with your doctor immediately if any of the following side effects occur:
Other side effects not listed above may also occur in some patients. If you notice any other effects, check with your doctor.
In October, 2023, treatment with cyclophosphamide, carfilzomib, and dexamethasone stopped working. My PET scan lit up like a Christmas tree. My lab results suddenly looked awful. I needed a unit of blood.

After starting another treatment, I had a quick response, and lab results returned to nearly normal levels. Normal for me.
Right now, I’m getting cyclophosphamide (Cytoxan), carfilzomib (Kyprolis), and dexamethasone every week. I’m tolerating it very well. Even though I had it in 2019 and eventually relapsed, it’s working for me.
After this, I’m hoping to try TAK-573 in a clinical trial.
Abstract
Background TAK-573, a humanized, anti-CD38, IgG4, monoclonal antibody genetically fused to two attenuated IFN?2b molecules, was designed for targeted delivery of attenuated IFN?2b to CD38 expressing (CD38+) cells, utilizing a unique epitope of CD38 that does not compete with current anti-CD38 therapies. Preclinical evaluation of TAK-573 confirmed activation of type I IFN signaling in CD38+ cells inducing direct anti-proliferative effects on multiple myeloma (MM) cells and direct and indirect immune cell activation. Here we provide the preliminary analyses of the pharmacodynamic data currently available from the ongoing Ph I/II TAK-573-1501 clinical study in patients with relapsed/refractory MM (NCT03215030).
Collins, Sabrina, et al. “357?TAK-573, an Anti-cd38–Attenuated Interferon Alpha (Ifn?) Fusion Protein (Attenukine™), Has Demonstrated Ifn? Receptor (IFNAR) Pathway Modulation in Patients with Relapsed/Refractory Multiple Myeloma.” Journal for ImmunoTherapy of Cancer, BMJ Specialist Journals, 1 Nov. 2020, https://jitc.bmj.com/content/8/Suppl_3/A218.1.
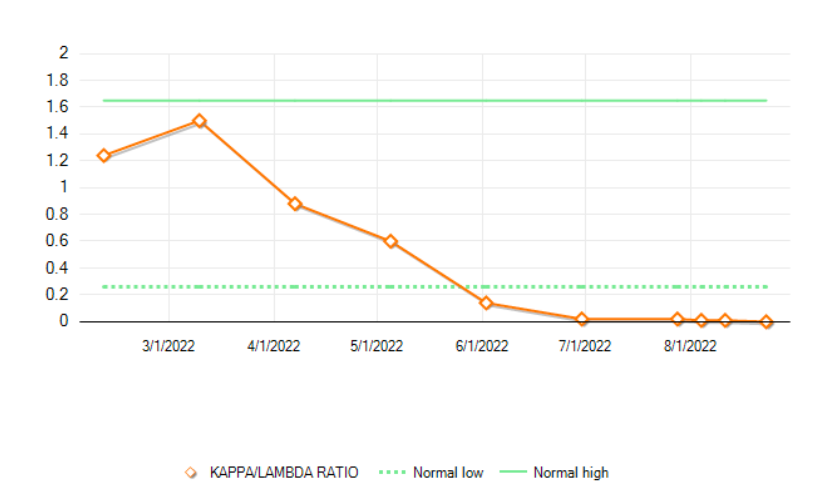
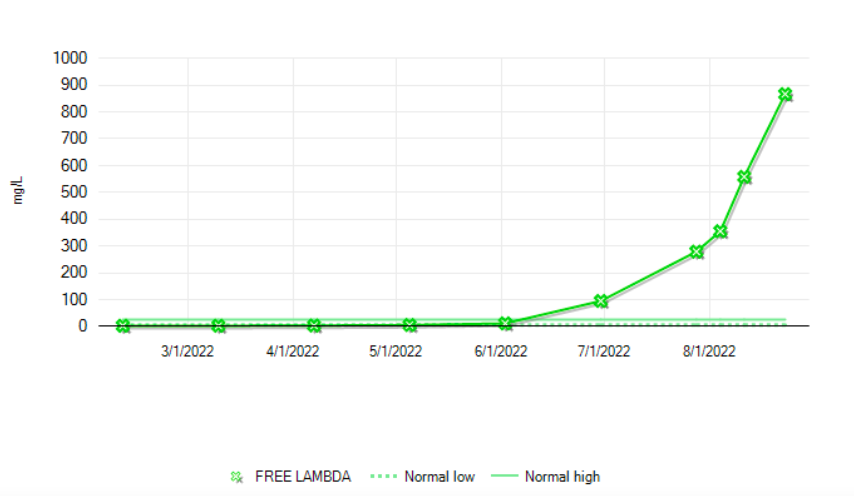
It’s been a while since I wrote. I began relapsing during the talquetamab/daratumumab/pomalidomide trial. I participated for about a year. The drugs worked for a good while – from June, 2021 until May, 2022.
Here are graphs of the free light chains (ratio and free lambda)
I have an appointment on September 20th to discuss the possibility of CAR T-Cell Therapy. Right now, I’m doing bridge therapy. Cyclophosphamide, carfilzomib, and dexamethasone. I’ve had this before, but I did relapse while on it. I hope it gets me through!
During cycle 5, the study team was given some freedom to adjust my dose of dexamethasone. We could do anything, from eliminating it completely to decreasing it. For 3 cycles, I was having 40 mg of dex a week. Dex is rough. If you have taken 40 mg of dex for any amount of time, you know what I mean.
I tried no dex at all, and I ended up having a fever because of CRS (cytokine release syndrome). The next week I took 10 mg of dex to tamp down my immune system just a little. I still had fevers. So, this week I’m back at 40. This sounds crazy, but I would rather have a fever than take dexamethasone.
My nails are improving, so that’s nice. I now have one really good nail on my left index finger. That’s the one I can use to open cans. I’ve taken my finger nails for granted my entire life. The other nails are growing out from the bottom, so it’s only the very tops that tend to be splintery and need to be kept trimmed so they don’t catch on things.
My sense of taste has not improved. Everything still tastes watered down. There are still things I can’t taste at all. Yellow mustard is one of those things. Another thing I can’t taste is butter. If I have buttered toast, it tastes like toasted bread with Crisco on it. It’s not worth it.
I still have a sensitivity to heat. That hasn’t changed at all. I’m glad summer is behind me, and I don’t have to be tethered to a fan and/or air conditioning. Doing chores around the house will still cause me to get too hot and get that uncomfortable feeling of electrical zaps to my head.
I have occasional itchy scalp. This was the worst on the week when I had not taken any dexamethasone. It’s crazy-making!
After work last weekend, I stopped to take a look at a covered bridge that’s on the way home. This is the Pisgah covered bridge. I was curious about why covered bridges were built, so I looked it up. According to Wikipedia, they were built that way to improve durability. A covered bridge could last up to 100 years.

Well, the daratumumab and pomalyst train has left the station without me. My doctor decided that it wasn’t helping me anymore, so I’ve moved on.
A few weeks ago I started carfilzomib (Kyprolis) and cyclophosphamide (Cytoxan). I also have 20 mg of dexamethasone every week. I have carfilzomib on Thursdays and Fridays and Cytoxan only on Thursdays. I’ll have three weeks on, then one week off. So far, my CBCs are pretty good. I have only slightly low hgb, rbc and platelets. Those were all low most of the time before this, anyway, so that’s nothing new.
As soon as I have some test results to post, I’ll do that.
If you’ve been on this treatment, I’d like to hear from you.
It’s been ages since I posted, but that’s because there’s been nothing new to report.
I recently began treatment with one of the new-ish monoclonal antibodies called Darzalex (daratumumab, aka dara). In addition to Darzalex, I’m taking an older drug that I’ve used before, called Revlimid. Once a week, I take a 20mg dose of dexamethasone.
It had been a little more than 9 years since I had any treatment for myeloma. After a stem cell transplant in 2007, I had no need for treatment. My disease stayed pretty stable for several years. Then, about 3 years ago, I began to relapse a little more noticeably. Finally, my doctor thought it was necessary to start treatment before I started to exhibit any symptoms. Only recently, my RBCs dipped below normal.
 I’ve had two infusions of dara so far. the first one took several hours to complete because of an infusion reaction. My blood pressure shot up to 203/97 and I developed a wheeze. The treatment was stopped for a while, and then the infusion was resumed at a lower rate. I was at the clinic for almost 12 hours that day. I’ll write more about that in a future post.
I’ve had two infusions of dara so far. the first one took several hours to complete because of an infusion reaction. My blood pressure shot up to 203/97 and I developed a wheeze. The treatment was stopped for a while, and then the infusion was resumed at a lower rate. I was at the clinic for almost 12 hours that day. I’ll write more about that in a future post.
As for Revlimid, I had that in 2006. It did very little for me, but I’m on it because my insurance company won’t pay for Pomalyst. This is because the dara/pom combination is considered “off-label” use. The price tag for Rev is about $11k per month, and Pom is about $13k per month. My clinic has billed about $45k for each infusion of dara. It’s hard to imagine, really!
Another first for me is that I’ve had a port implanted to handle the frequent infusions. It was an outpatient procedure. I was in at 7:15 Friday morning and out by 10:30 am. There’s some discomfort, but it’s not terrible. The surgeon prescribed some norco tablets. He even gave me a prescription for a lidocaine gel to apply before port accesses to numb the area before the needle is inserted.
That’s it for me now. I’ll provide some more details in future posts.